NCC US 022218
/CASE 1: 55 yom, history of GBM, 3 weeks post resection, presents to ED with SOB and hypotension and hypoxia. What does the US show and what is the treatment?
US demonstrates the classic findings of acute RV afterload increase consistent with the diagnosis of massive PE and right hear strain. McConnell’s sign is present (from our friends at EMORY: McConnell's Sign)
Treatment in this case was the placement of an EKOS catheter (EKOS catheter) for local administration of fibrinolytics to limit the systemic exposure and risk of hemorrhage into the surgical bed. The patient recovered and was discharged from the NSICU to rehab.
CASE 2: Coagulopathic 65 yof with IGM nephropathy needing central access. Challenging access of RIJ. How do you confirm intravascular wire placement prior to dilation of the vessel?
Longitudinal view of intravascular wire with linear array transducer demonstrates proper location of wire and procedure is safe to continue
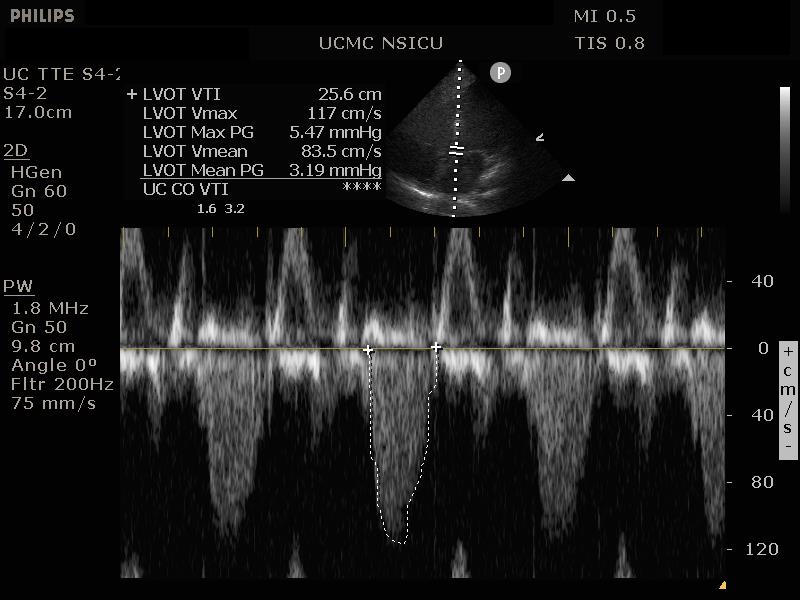
CASE 3: Hypotensive 60 yof on a norepinephrine infusion with MAP < 60 mmHg. How do you objectively asses LV function with ECHO?
US demonstrates the classic findings of acute RV afterload increase consistent with the diagnosis of massive PE and right hear strain. McConnell’s sign is present (from our friends at EMORY: McConnell's Sign)
Treatment in this case was the placement of an EKOS catheter (EKOS catheter) for local administration of fibrinolytics to limit the systemic exposure and risk of hemorrhage into the surgical bed. The patient recovered and was discharged from the NSICU to rehab.